Living with COVID and keeping your choir viable while you’re at it. As has been the case throughout this pandemic, your choir must abide by the public health regulations in force at any time. The challenge arising for WA choirs is that we haven’t lived with COVID at all as yet and the fear of doing so, or the reality of doing so, may impact on your choir members in ways that adversely impact the viability of your choir in this phase of opening up to the rest of the country and the world.
Our goal is to assist you and the broader singing community to prepare for this phase, as best you can, while we are still COVID-free and have some time to work through some potentially complex issues in a considered way.
The published public health restrictions planned for WA when we reach the point on 90% full vaccination of the population over the age of 12 are detailed in the “Fact to Share” section below. These will have almost no impact on your ability to rehearse and perform as you are currently doing. The issue that choirs and individual singers have to grapple with is what measures your particular choir feel is appropriate, if any, over and above these restrictions, to address the risk of choir members contracting COVID in the choir setting once COVID is circulating in the WA community.
Every person will perceive the risk that COVID represents to them differently and will have different risk thresholds. Ideally you want to work with your members to arrive at an agreed approach such that your members are comfortable that coming to choir represents an equivalent or lower risk to their wellbeing than undertaking other activities that they are also prepared to continue doing once COVID arrives. You are not striving for or promising zero risk of infection. That’s a promise you can’t keep. You are assisting your members to develop an awareness of the risks they face in every aspect of their lives and to mentally prepare to live with COVID.
The peak bodies for choirs in WA can not and will not mandate specific approaches that every choir should take. This is a matter of individual choice and the collective approach of the specific group of individuals that currently make up your singing group and new members you will attract in the future. However we will provide you with a “shopping list” of measures that your choir should consider and adopt, or not, as your members consider appropriate for their perceived vulnerability and appetite for risk. We will also provide you with another list of scenarios that your members can consider to determine what your group agree to be the most appropriate response should such situations arise for your members in the future. These could form the basis for a series of discussions which will lead to guidelines which you can share with all your current and future members.
Obviously you will be striving to arrive at solutions that suit the needs of the vast majority of your existing members. The willingness of people to be open to the needs of others and accept compromise will assist this and will require some skilful dialogue and, potentially, the sharing of some facts as a basis for these discussions. We have prepared such a fact sheet that we believe represents a reasonable summary of the currently accepted facts as published by reputable health authorities which you may choose to share with your choir members if you see fit.
Having done all this there is still a chance that you will discover that a significant minority of your members have concerns that are unable to be addressed by consensus. In the opinion of the peak community singing bodies in WA, it is most important that choirs continue to survive and prosper through these challenging phases. If your choir discovers that it is going to be challenged through a potential loss of membership, a need to invest in new technology, a need for a new rehearsal venue etc, etc, this is important information for your choir to grapple with sooner than later so that mitigation plans can be put in place and assistance sought.
Your peak singing bodies, Voice Moves WA, SongFest Inc and ANCA (WA) will seek to share information, provide support and make representation as appropriate in support of choirs that identify specific concerns. Please take the opportunity to prepare your choir now and get the conversations started. COVID is coming and we in WA are uniquely fortunate in the world to have some time to prepare. Please use that opportunity.
How Exactly Do You Catch Covid-19? There Is a Growing Consensus
Surface contamination and fleeting encounters are less of a worry than close-up, person-to-person interactions for extended periods
Six months into the coronavirus crisis, there’s a growing consensus about a central question: How do people become infected?
It’s not common to contract Covid-19 from a contaminated surface, scientists say. And fleeting encounters with people outdoors are unlikely to spread the coronavirus.
Instead, the major culprit is close-up, person-to-person interactions for extended periods. Crowded events, poorly ventilated areas and places where people are talking loudly—or singing, in one famous case—maximize the risk.
These emerging findings are helping businesses and governments devise reopening strategies to protect public health while getting economies going again. That includes tactics like installing plexiglass barriers, requiring people to wear masks in stores and other venues, using good ventilation systems and keeping windows open when possible.
Two recent large studies showed that wide-scale lockdowns—stay-at-home orders, bans on large gatherings and business closures—prevented millions of infections and deaths around the world. Now, with more knowledge in hand, cities and states can deploy targeted interventions to keep the virus from taking off again, scientists and public-health experts said.
“We should not be thinking of a lockdown, but of ways to increase physical distance,” said Tom Frieden, chief executive of Resolve to Save Lives, a nonprofit public-health initiative. “This can include allowing outside activities, allowing walking or cycling to an office with people all physically distant, curbside pickup from stores, and other innovative methods that can facilitate resumption of economic activity without a rekindling of the outbreak.”
The group’s reopening recommendations include widespread testing, contact tracing and isolation of people who are infected or exposed.
A Recipe for Infection
Getting the Covid-19 virus involves three steps.
1 Coughing, talking and breathing creates virus-carrying droplets of various sizes.
2 Enough virus has to make itself over to you or build up around you over time to trigger an infection.
3 The virus has to make its way into your respiratory tract and use the ACE-2 receptors there to enter cells and replicate.
One important factor in transmission is that seemingly benign activities like speaking and breathing produce respiratory bits of varying sizes that can disperse along air currents and potentially infect people nearby.
Health agencies have so far identified respiratory-droplet contact as the major mode of Covid-19 transmission. These large fluid droplets can transfer virus from one person to another if they land on the eyes, nose or mouth. But they tend to fall to the ground or on other surfaces pretty quickly.
Some researchers say the new coronavirus can also be transmitted through aerosols, or minuscule droplets that float in the air longer than large droplets. These aerosols can be directly inhaled.
That’s what may have happened at a restaurant in Guangzhou, China, where an infected diner who was not yet ill transmitted the virus to five others sitting at adjacent tables. Ventilation in the space was poor, with exhaust fans turned off, according to one study looking at conditions in the restaurant.
Aerosolized virus from the patient’s breathing or speaking could have built up in the air over time and strong airflow from an air-conditioning unit on the wall may have helped recirculate the particles in the air, according to authors of the study, which hasn’t yet been peer-reviewed.
Sufficient ventilation in the places people visit and work is very important, said Yuguo Li, one of the authors and an engineering professor at the University of Hong Kong. Proper ventilation—such as forcing air toward the ceiling and pumping it outside, or bringing fresh air into a room—dilutes the amount of virus in a space, lowering the risk of infection.
A gym in Chino Hills, Calif., on June 12. PHOTO: WILL LESTER/ORANGE COUNTY REGISTER/ZUMA PRESS
Another factor is prolonged exposure. That’s generally defined as 15 minutes or more of unprotected contact with someone less than 6 feet away, said John Brooks, the Centers for Disease Control and Prevention’s chief medical officer for the Covid-19 response. But that is only a rule of thumb, he cautioned. It could take much less time with a sneeze in the face or other intimate contact where a lot of respiratory droplets are emitted, he said.
Superspreaders
At a March 10 church choir practice in Washington state, 87% of attendees were infected, said Lea Hamner, an epidemiologist with the Skagit County public-health department and lead author of a study on an investigation that warned about the potential for “superspreader” events, in which one or a small number of people infect many others.
Members of the choir changed places four times during the 2½-hour practice, were tightly packed in a confined space and were mostly older and therefore more vulnerable to illness, she said. All told, 53 of 61 attendees at the practice were infected, including at least one person who had symptoms. Two died.
Several factors conspired, Ms. Hamner said. When singing, people can emit many large and small respiratory particles. Singers also breathe deeply, increasing the chance they will inhale infectious particles.
Similar transmission dynamics could be at play in other settings where heavy breathing and loud talking are common over extended periods, like gyms, musical or theater performances, conferences, weddings and birthday parties. Of 61 clusters of cases in Japan between Jan. 15 and April 4, many involved heavy breathing in close proximity, such as karaoke parties, cheering at clubs, talking in bars and exercising in gyms, according to a recent study in the journal Emerging Infectious Diseases.
The so-called attack rate—the percentage of people who were infected in a specific place or time—can be very high in crowded events, homes and other spaces where lots of people are in close, prolonged contact.
An estimated 10% of people with Covid-19 are responsible for about 80% of transmissions, according to a study published recently in Wellcome Open Research. Some people with the virus may have a higher viral load, or produce more droplets when they breathe or speak, or be in a confined space with many people and bad ventilation when they’re at their most infectious point in their illness, said Jamie Lloyd-Smith, a University of California, Los Angeles professor who studies the ecology of infectious diseases.
But overall, “the risk of a given infected person transmitting to people is pretty low,” said Scott Dowell, a deputy director overseeing the Bill & Melinda Gates Foundation’s Covid-19 response. “For every superspreading event you have a lot of times when nobody gets infected.”
The attack rate for Covid-19 in households ranges between 4.6% and 19.3%, according to several studies. It was higher for spouses, at 27.8%, than for other household members, at 17.3%, in one study in China.
Rosanna Diaz with her son Tomas. PHOTO: ROSANNA DIAZ
Rosanna Diaz lives in a three-bedroom apartment in New York City with five other family members. The 37-year-old stay-at-home mother was hospitalized with a stroke on April 18 that her doctors attributed to Covid-19, and was still coughing when she went home two days later.
She pushed to get home quickly, she said, because her 4-year-old son has autism and needed her. She kept her distance from family members, covered her mouth when coughing and washed her hands frequently. No one else in the apartment has fallen ill, she said. “Nobody went near me when I was sick,” she said.
Being outside is generally safer, experts say, because viral particles dilute more quickly. But small and large droplets pose a risk even outdoors, when people are in close, prolonged contact, said Linsey Marr, a Virginia Tech environmental engineering professor who studies airborne transmission of viruses.
No one knows for sure how much virus it takes for someone to become infected, but recent studies offer some clues. In one small study published recently in the journal Nature, researchers were unable to culture live coronavirus if a patient’s throat swab or milliliter of sputum contained less than one million copies of viral RNA.
What to Expect When Flying Now (and in the Future)
Air travel is full of opportunities for coronavirus transmission. Touchless check-in, plexiglass shields, temperature checks, back-to-front boarding and planes with empty middle seats are all now part of the flying experience, and the future may bring even more changes. Illustration: Alex Kuzoian
“Based on our experiment, I would assume that something above that number would be required for infectivity,” said Clemens Wendtner, one of the study’s lead authors and head of the department of infectious diseases and tropical medicine at München Klinik Schwabing, a teaching hospital at the Ludwig Maximilian University of Munich.
He and his colleagues found samples from contagious patients with virus levels up to 1,000 times that, which could help explain why the virus is so infectious in the right conditions: It may take much lower levels of virus than what’s found in a sick patient to infect someone else.
Changing policies
Based on this emerging picture of contagion, some policies are changing. The standard procedure for someone who tests positive is to quarantine at home. Some cities are providing free temporary housing and social services where people who are infected can stay on a voluntary basis, to avoid transmitting the virus to family members.
The CDC recently urged Americans to keep wearing masks and maintaining a distance from others as states reopen. “The more closely you interact with others, the longer the interaction lasts, the greater the number of people involved in the interaction, the higher the risk of Covid-19 spread,” said Jay Butler, the CDC’s Covid-19 response incident manager.
If the number of Covid-19 cases starts to rise dramatically as states reopen, “more extensive mitigation efforts such as what were implemented back in March may be needed again,” a decision that would be made locally, he said.
CDC guidelines for employers whose workers are returning include requiring masks, limiting use of public transit and elevators to reduce exposure, and prohibiting hugs, handshakes and fist-bumps. The agency also suggested replacing communal snacks, water coolers and coffee pots with prepacked, single-serve items, and erecting plastic partitions between desks closer than 6 feet apart.
A crowd gathered at a bar in Columbus, Ohio, on May 15. PHOTO: DORAL CHENOWETH/THE COLUMBUS DISPATCH/ASSOCIATED PRESS
Current CDC workplace guidelines don’t talk about distribution of aerosols, or small particles, in a room, said Lisa Brosseau, a respiratory-protection consultant for the University of Minnesota’s Center for Infectious Disease Research and Policy.
“Aerosol transmission is a scary thing,” she said. “That’s an exposure that’s hard to manage and it’s invisible.” Ensuring infected individuals stay home is important, she said, but that can be difficult due to testing constraints. So additional protocols to interrupt spread, like social distancing in workspaces and providing N95 respirators or other personal protective equipment, might be necessary as well, she said.
Some scientists say while aerosol transmission does occur, it doesn’t explain most infections. In addition, the virus doesn’t appear to spread widely through the air.
“If this were transmitted mainly like measles or tuberculosis, where infectious virus lingered in the airspace for a long time, or spread across large airspaces or through air-handling systems, I think you would be seeing a lot more people infected,” said the CDC’s Dr. Brooks.
Sampling the air in high-traffic areas regularly could help employers figure out who needs to get tested, said Donald Milton, professor of environmental and occupational health at the University of Maryland School of Public Health.
“Let’s say you detect the virus during lunchtime on Monday in a dining hall,” he said. “You could then reach out to people who were there during that time telling them that they need to get tested.”
Erin Bromage, a University of Massachusetts Dartmouth associate professor of biology, has been fielding questions from businesses, court systems and even therapists after a blog post he wrote titled “The Risks—Know Them—Avoid Them” went viral.
Courts are trying to figure out how to reconvene safely given that juries normally sit close together, with attorneys speaking to them up close, Dr. Bromage said. Therapists want to be able to hold in-person counseling sessions again. And businesses are trying to figure out what types of cleaning and disease-prevention methods in which to invest most heavily.
He advises that while wiping down surfaces and putting in hand-sanitizer stations in workplaces is good, the bigger risks are close-range face-to-face interactions, and having lots of people in an enclosed space for long periods. High-touch surfaces like doorknobs are a risk, but the virus degrades quickly so other surfaces like cardboard boxes are less worrisome, he said. “Surfaces and cleaning are important, but we shouldn’t be spending half of our budget on it when they may be having only a smaller effect,” he said.
Plexiglass dividers at the Bellagio Hotel and Casino in Las Vegas on June 4. PHOTO: JOE BUGLEWICZ/BLOOMBERG NEWS
Drugmaker Eli Lilly & Co. has a medical advisory panel that’s reading the latest literature on viral transmission, which it is using to develop recommendations for bringing back the company’s own workers safely.
To go into production facilities, some of which are in operation now, scientists must don multiple layers of personal protective equipment, including gloves, masks, goggles and coveralls. That’s not abnormal for drug-development settings, said Lilly Chief Scientific Officer Daniel Skovronsky. “The air is extensively filtered. There’s lots of protection,” he said.
The places he worries about are the break rooms, locker rooms and security checkpoints, where people interact. Those are spaces where the company has instituted social-distancing measures by staggering the times they are open and how many people can be there at once. Only a few cafeterias are open, and those that are have socially distanced seating. In bathrooms, only half the stalls are available to cut down on the number of people.
“We’ll never be more open than state guidelines,” Dr. Skovronsky said, but “we’re often finding ourselves being more restrictive because we’re following the numbers.”
Globally, health-care authorities are searching for effective measures to prevent community transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Although data on factors related to this transmission are scarce, the spread of SARS-CoV-2 is thought to mostly be via the transmission of respiratory droplets coming from infected individuals.1 Small droplets, from submicron to approximately 10 μm diameter, produced during speech and coughing, have been shown to contain viral particles,2 which can remain viable and infectious in aerosols for 3 h.3 The droplets can be transmitted either directly by entering the airway through the air (aerosols),4 or indirectly by contact transfer via contaminated hands. The mode of transmission could affect whether an infection starts in the upper or lower respiratory tract, which is thought to affect the severity of the disease progression.5 Notably, the dose–response relationship of SARS-CoV-2 infection is still unclear, especially with respect to aerosol transmission of the virus. However, aerosols containing a small concentration of virus in poorly ventilated spaces, combined with low humidity and high temperature,6 might result in an infectious dose over time.
To better understand the spreading of respiratory droplets and possible preventive measures, we analysed droplet production due to coughs and speech by measuring the droplet size distribution, travel distance and velocity, and the airborne time in relation to the level of air ventilation.
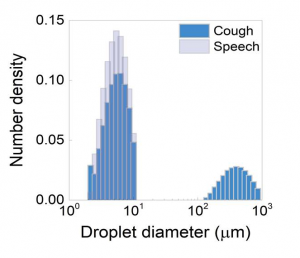
We did a laser diffraction measurement using a spray droplet measurement system (Malvern Spraytec, Malvern, UK) to determine the size distribution of respiratory droplets in a single cough and during speech. In a cough from a healthy volunteer, we found two distinct types of drops, large droplets (100–1000 μm in diameter) and small droplets (1–10 μm), with the small droplets being much more prevalent (appendix p 1). During speech, only the small droplets were found (appendix p 1). Although large droplets have been specifically related to coughs,4 here we observe that both sizes of droplet are produced by coughing.
appendix p 1
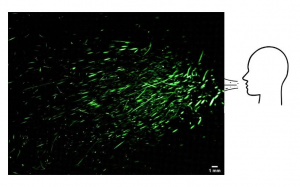
Next, we used a SprayScan (Spraying Systems, Glendale Heights, IL, USA) laser sheet to track droplets by filming the scattering of laser light by droplets from a cough7 to determine the speed of the droplets and their trajectory. Large droplets were observed to fall onto the ground rapidly (appendix p 2). We found that although the speed of the drops ranged 2–7 m/s at the start of the cough, the visible large drops (typically 500 μm in diameter) do not travel far before their trajectory bends down due to gravity to rapidly fall onto the ground within 1 s. This observation can be explained by balancing the forces of gravity (F=mg; where F is force, m is mass, and g is acceleration) and air drag (F=6πηRU, in which η is the air viscosity, R is the radius of the droplet, and U is the falling velocity), from which it also follows that the small droplets of typical radius of 5 μm will take 9 min to reach the ground when produced at a height of 160 cm (ie, average speaking or coughing height). These small droplets are of specific interest because they have been associated with aerosol transmission of the SARS-CoV-2.8 We also investigated droplets coming from the nasal cavity, and found that with normal breathing no droplets are detected above the background noise level (2·3 [SD 1·5] droplets, and 2·6 [1·7] droplets for nasal breathing). From a sneeze, we found mostly very large drops, originating from both the buccal and nasal cavities, that are not persistent.
appendix p 2
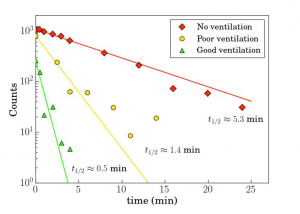
The same laser sheet was used to investigate how long small droplets from a cough will float through the air. We used a specially designed spray nozzle from Medspray (Enschede, The Netherlands) to disperse a controlled quantity of small droplets into the air, reproducing the effect of coughing. The droplets have an average diameter of 5 μm and are dispersed homogeneously by the spray nozzle. We analysed the number of droplets passing through the stationary laser sheet suspended in the centre of the experimental chamber using an algorithm that detects the illuminations caused by the droplets. We repeated this experiment in three rooms with different levels of ventilation: no ventilation, mechanical ventilation only, and mechanical ventilation supported by the opening of an entrance door and a small window (appendix p 3). In the best ventilated room, after 30 s the number of droplets had halved, whereas with no ventilation this took about 5 min, in agreement with the air drag calculation that shows that 5 μm drops from the average cough or speech height take 9 min to reach the ground. In a poorly ventilated room, the number of droplets was halved in 1·4 min.
appendix p 3
Although we only studied healthy volunteers and did not study patients with COVID-19 or virus-laden aerosol droplets directly, our data on droplet size distribution and persistence does have implications on requirements to use face masks to prevent virus transmission. Transmission by aerosols of the small droplets studied here can only be prevented by use of high-performance face masks; a conventional surgical mask only stops 30% of the small aerosol droplets studied here for inhaled breath;9 for exhaled breath the efficacy is much better.10
Additionally, the long airborne time of aerosols we found here affects the reliability of temporal and spatial contact data between individuals as monitored by proximity tracing via smartphone apps. These findings need to be considered in the development and implementation of these apps.
This study shows that better ventilation of spaces substantially reduces the airborne time of respiratory droplets. This finding is relevant because typically poorly ventilated and populated spaces, like public transport and nursing homes, have been reported as sites of viral transmission despite preventive physical distancing. The persistence of small respiratory droplets in such poorly ventilated spaces could contribute to the spread of SARS-CoV-2. Our findings confirm that improving ventilation of public spaces will dilute and clear out potentially infectious aerosols. To suppress the spread of SARS-CoV-2 we believe health-care authorities should consider the recommendation to avoid poorly ventilated public spaces as much as possible. The implications are also important for hospital settings where aerosolisation by coughing and medical treatments and close contact with COVID-19 patients is very common.
SongFest Inc is a not for profit organisation with the aim of promoting community singing in Western Australia. To date, SongFest’s most visible work has been in organising or facilitating festivals for singing groups.
Suddenly, and quite unexpectedly, the COVID pandemic seriously challenges community singing in WA, as everywhere. The aim of this document is to share information relevant to directors and managers of choirs to assess how they could resume live rehearsals. It also presents ideas that may assist choir managers to decide whether, when and how to resume rehearsals. The discussion will be ongoing as the virus’ spread is managed in WA and as more information comes to light about the virus in general and its relationship to singing.
This document is not intended as scientific or medical advice. We cannot find any studies that are directly related to the spread of COVID by group singing activities. Consequently there is no certainty or assurance of safety that can be given to participants in group singing. In fact, quite the opposite. Singing, like most activities, represents a risk of virus spread.
Does that mean that community singing needs to come to a halt in WA until a vaccine is developed? Singers who are vulnerable to complications from COVID infection may well decide so. Others may decide to sing. Singers can evaluate risks from an informed position and act to maximise their chances of avoiding infection and infecting others when they do rehearse.
Higher risk people
Singers who fall within the high-risk categories for complications with COVID need to decide if they should undertake any high-risk contact activities, including singing. Group rehearsals in any circumstances will entail some level of risk. Details of high-risk people are detailed in the link below for your information.
Risks that may be associated with singing rehearsals and events and the basis for this association
We note the concern regarding group singing based upon a number of clusters identified in several countries where singing groups, rehearsing without precautions or with partial precautions, experienced very high levels of cross-infection attributed to a single rehearsal. The CDC report into the Washington choir cluster can be read here https://www.cdc.gov/mmwr/volumes/69/wr/mm6919e6.htm
This has led health authorities to believe that some aspect of the “normal” singing can make singers “super spreaders”. The exact mechanism is not known. It may be a combination of:
greater proportion of droplets and aerosols (which can contain the virus) by singing compared to talking
Larger numbers of people generating thermal mixing of the air in the rehearsal space which spread the aerosols throughout the space to a greater extent
Aspects of the volume of the rehearsal space, the extent to which singers are facing each other, the amount of natural ventilation, use of air conditioning recirculating air and impact of overhead fans
The age of the singers
The relatively long period of contact across a rehearsal
Socialisation and refreshments associated with tea breaks
The WA Health Department have been approached directly by ANCA regarding the health risks of singing. The advice received from Dr Revle Bangor-Jones Coordinator – (WA) Public Health Emergency Operation Centre was;
“Phase 3 of the COVID-19 WA roadmap allows for indoor and outdoor gatherings of up to 100 people at any one time, per single undivided space, and applying the revised two square metre per person capacity rule. School choirs in WA have recommenced.
Everyone is encouraged to continue to practice physical distancing and good personal hygiene and minimise the use of any shared equipment. Shared equipment should be cleaned between use.”
This indicates that singing isn’t considered by WA Public Health to be special as an activity at this stage.
Research on the longevity of the virus on surfaces and in the air indicates that dark, cool, dry environments maximise the viability of the virus while exposure to sunlight and humidity dramatically reduces the half-life of the virus. The use of cleaning agents which destroy the fatty layer surrounding the virus are the most effective.
The effectiveness of masks is impaired by the duration of use (30 minutes is considered an upper bound beyond which the buildup of moisture on the mask enables aerosols to be generated through the mask), touching the mask with hands, incorrect removal and application (by the straps, not the fabric) and by the volume of air generated by the user.
Risk Mitigation
Groups with singers who are prepared to accept the level of risk associated with group singing will want to act to maximise the protection of their close contacts should their singing activity ultimately result in an infection.
A key tool to mitigating the risk of infection of close contacts of singers is to utilise the COVID Safe App or for choirs to keep a record of all rehearsal attendees. In Australia we have bought time through our national lockdown to enable us to prepare and boost our testing and contact tracing capability. Our ability to gather together with reduced social distancing and open our community to the rest of the country and to the world, depends on rapid identification and isolation of new infections and isolation of all close contacts. This process will be greatly enhanced by the adoption of the app and singers can lead the way to assist widespread acceptance of our “high-risk” activity.
Factors which may help reduce infection risk during rehearsal may include:
Higher spacing between singers.
Participant numbers – other mitigation strategies can be enhanced as numbers increase. For instance, making some rehearsals sectional only would limit the number of times the whole group comes together.
Outdoor rehearsals — these offer the benefits of natural ventilation and sunshine, which has been shown to reduce the viral load.
Shorter Singing aspects of the rehearsal could be focused.
Separate singing and socialising: Non-singing aspects of the rehearsal could be conducted in a different space. Groups can avoid conducting refreshments in the rehearsal space. Practice high levels of personal hygiene around all sharing of food, drink and utensils.
Practice hand hygiene before and after singing phases of the rehearsal.
Chairs can be set out, stacked and cleaned by a small number of people practicing social distancing rather than having everybody congregating and milling around.
Singers who are at high risk of serious outcomes with COVID face a difficult period in terms of live singing. Consider streaming the group’s rehearsals and having high risk members participate on a screen in the rehearsal space.
Some final thoughts: Western Australian conditions
At the time of writing there is little risk in live rehearsals because in WA we have almost no COVID community transmission. However, this is a marathon, not a sprint. The virus may represent a health risk for years to come. A plan to keep singing when modest levels of community transmission are identified is a key goal that choirs should consider. Do you stop as soon as community transmission is detected or does your group bring in some additional mitigation measures and keep singing together?
Other choir organisations around the world are still seeing significant community transmission and may still be some way from getting back to live rehearsals. Can we develop approaches here which will help choirs in other countries get back to singing together?
Strategies for returning to Sing with and without COVID
Summary of comments from Webinar No.1 by Tim Fisher
Feedback from 62 choirs indicates that:
We need to change the dialogue with our members from certainty and safety to managed risk and quick response consistent with living with COVID-19 for the long term. The risks posed by aerosols, spacing, ventilation etc, etc cannot be quantified and cannot be eliminated and it is not your job to do so.
Choir managers should be confident that they are acting responsibly when they comply with the current state government health regulations. Singing isn’t special when it comes to group activities in a pandemic. Every activity has risk. WA Health Dept advice received by ANCA 2 weeks ago confirms that they have no special concerns about singing at this stage.
Assisting all singers to make an informed choice about the risks they face when they attend choir rehearsals is a key objective for choir managers. Vulnerable singers may choose to attend live rehearsals now and they may not. They may choose to keep attending live rehearsals even when community transmission of the virus reappears in WA and they may not. Your job is not to persuade anyone to keep singing. Your job is to help your choir comply with the current health regulations to give vulnerable singers confidence that your choir take their risk seriously and to discover what measures that the whole choir needs to adopt would make your vulnerable singers feel that the risks involved were acceptable in the future.
Each choir should consider implementing their own COVID Safety Plan to reflect these strategies and share information to enable this decision.
Mitigation (not elimination) of risk and effective contact tracing and isolation are the primary aims
Measures to meaningfully engage with your vulnerable members are an integral part of your plan but may not involve live rehearsals for some. Shared information and agreed strategies will maximise ongoing engagement, even when community transmission appears. Your vulnerable singers need your support. With COVID the most vulnerable to complications from catching the disease are also generally the most vulnerable to not having the technical or financial capability to maintain an online connection with your group. How can you maintain a meaningful and hopefully tuneful connection with all your members? Is now the time to be launching a recruitment drive for new singers?
Behaviour change will be required to ensure that all singers conform to the plan, particularly now when most people believe there is no risk. You need to assist all your singers with training and you need to discuss acceptable ways to hold everyone accountable to sticking to that plan. This will require leadership.